[In Italy]
This case series describes COVID-19 symptoms persisting a mean of 60 days after onset among Italian patients previously discharged from COVID-19 hospitalization. We assessed persistent symptoms in patients who were discharged from the hospital after recovery from COVID-19.
Results
From April 21 to May 29, 2020, 179 patients were potentially eligible for the follow-up post acute care assessment; 14 individuals (8%) refused to participate and 22 had a positive test result. Thus, 143 patients were included. The mean age was 56.5 (SD, 14.6) years (range, 19-84 years), and 53 (37%) were women. During hospitalization, 72.7% of participants had evidence of interstitial pneumonia. The mean length of hospital stay was 13.5 (SD, 9.7) days; 21 patients (15%) received noninvasive ventilation and 7 patients (5%) received invasive ventilation. The characteristics of the study population are summarized in the Table.
Patients were assessed a mean of 60.3 (SD, 13.6) days after onset of the first COVID-19 symptom; at the time of the evaluation, only 18 (12.6%) were completely free of any COVID-19-related symptom, while 32% had 1 or 2 symptoms and 55% had 3 or more. None of the patients had fever or any signs or symptoms of acute illness. Worsened quality of life was observed among 44.1% of patients. The Figure shows that a high proportion of individuals still reported fatigue (53.1%), dyspnea (43.4%), joint pain, (27.3%) and chest pain (21.7%). 1
Lex Rutten MD
In the summer issue of AJHM the data collection project of the Liga Medicorum Homeopathica Internationalis (LMHI) was described.1 A new illness offers the opportunity to develop a new repertory with state-of-the-art statistical techniques and based on a solid mathematical principle: Bayes’ theorem.
The essential difference between the classical repertory and a Bayesian repertory is the use of prevalence instead of absolute occurrence. This is shown in Table 1: prevalence corrects for the unequal use of different homeopathic medicines (Arsenicum album, Bryonia alba, Gelsemium sempervirens, Phosphorus and Pulsatilla). In absolute numbers the symptom ‘cough’ was seen in 33 Arsenicum patients and in 14 Phosphorus patients. However, the prevalence of ‘cough’ was 38.4% in Arsenicum and 77.8% in Phosphorus. The complete database is comprised of 416 COVID-19 treatments that were evaluated as successful by the doctor. Most cases were entered via the American Institute of Homeopathy (AIH) database, others from the database of the Ärztegemeinschaft für Klassisiche Homoeopathie (AKH) and from individual case descriptions.
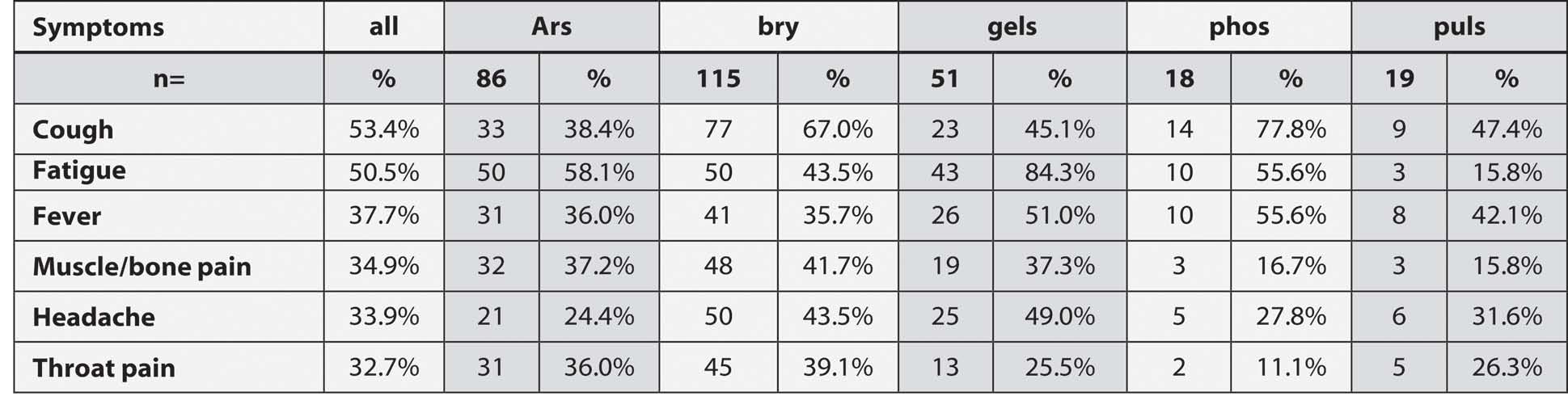
Table 1: Absolute occurrence and prevalence (%) of symptoms in the whole COVID-19 population (column ‘all’) and in populations responding to five homeopathic medicines: Arsenicum album (Ars), Bryonia alba (Bry), Gelsemium sempervirens (Gels), Phosphorus (Phos) and Pulsatilla (Puls).
Table 1 also shows a comparison between medicine populations and the whole population. Intuitively it is easy to understand that especially a prevalence above average is related to indications for specific medicines. This is expressed as likelihood ratio (LR) = (prevalence in medicine population) / (prevalence in the remainder of the population). LR is the core element of the Bayesian formula: Posterior odds = LR x prior odds. Table 2 shows a part of a Bayesian repertory of COVID-19 symptoms for five homeopathic medications mentioned above. These five medications were prescribed in 69.5% of all COVID-19 cases. LR>1 indicates that the symptom is an indication for the medication, LR<1 indicates that the symptom is a relative contraindication for the medication.
Table 1 also shows a comparison between medicine populations and the whole population. Intuitively it is easy to understand that especially a prevalence above average is related to indications for specific medicines. This is expressed as likelihood ratio (LR) = (prevalence in medicine population) / (prevalence in the remainder of the population). LR is the core element of the Bayesian formula: Posterior odds = LR x prior odds. Table 2 shows a part of a Bayesian repertory of COVID-19 symptoms for five homeopathic medications mentioned above. These five medications were prescribed in 69.5% of all COVID-19 cases. LR>1 indicates that the symptom is an indication for the medication, LR<1 indicates that the symptom is a relative contraindication for the medication.
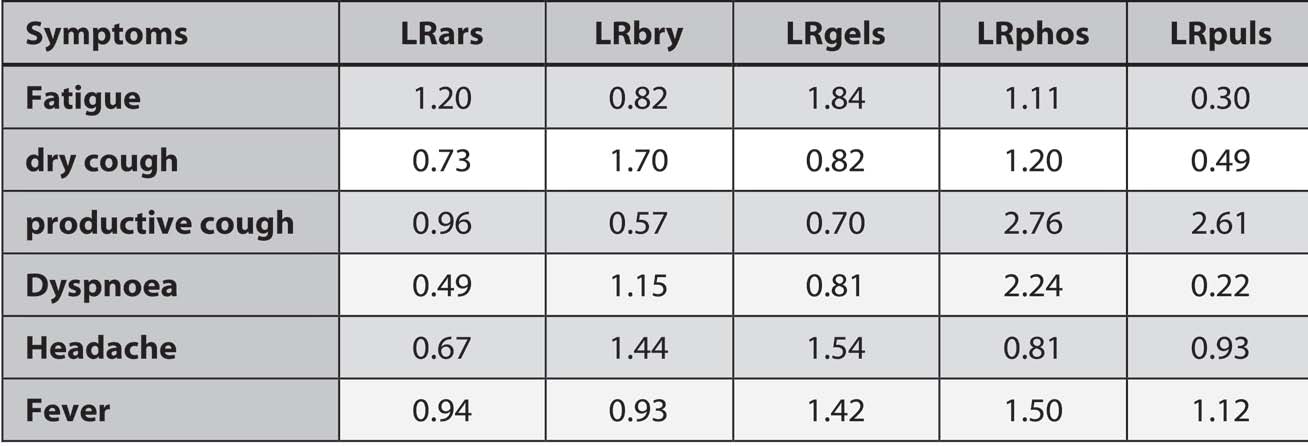
Table 2: Part of the Mini-Repertory for COVID-19 symptoms
The use of LR, and hence indication and contraindication, shows a clear difference between medicines for relatively common symptoms, a difference that would not be visible in the classical repertory. This difference between medicines becomes stronger if we combine symptoms. Table 3 shows that three common symptoms, fatigue, dry cough and dyspnea, differentiate well between Bry. and Phos. on the one hand, and Ars. and Puls. on the other hand.

Table 3: combined LR for five medicines and three symptoms (fatigue, dry cough, dyspnoea)
The downside of the Bayesian repertory is the need for calculations, but that can easily be resolved by the computer. For this purpose, Tom Smedley, Galen Ives and Lex Rutten developed an app that can be found at the internet address: https://hpra.co.uk/.
The app was tested with 17 well-described successful cases,2 and rendered nearly the same results with one-half to one-fourth of the symptoms necessary in classical repertorization.3
Experienced homeopathic practitioners can use the app to get an initial idea about possible medications with common COVID-19 symptoms. They will see that it provides information which has never been available to them before. It also reflects their own experience if they have contributed to the database.
Even more important might be showing the world that homeopathy is basically a reproducible method, supported by an algorithm. Probably the most unfortunate people in this pandemic are the elderly living in nursing homes. Homeopathic practitioners could reach out to doctors working in these homes by inviting them to try the app with their residents to select those most likely medications for homeopathic treatment. Then the homeopaths could complete the homeopathic anamnesis for these patients and instruct the doctors at the nursing homes how to administer the medication.
 About the author: Dr. Lex Rutten graduated in the Netherlands as a medical doctor in 1977, and as a General practitioner in 1978. He worked as a GP in his private practice for five years, but started homeopathic training in 1979, as well as training in philosophy, statistics and research methodology. From 1983 on, he has practised as a homeopathic physician. He has had many organisational functions in national and international homeopathic professional and educational organisations, and has been a teacher of homeopathy in postgraduate training for doctors.
About the author: Dr. Lex Rutten graduated in the Netherlands as a medical doctor in 1977, and as a General practitioner in 1978. He worked as a GP in his private practice for five years, but started homeopathic training in 1979, as well as training in philosophy, statistics and research methodology. From 1983 on, he has practised as a homeopathic physician. He has had many organisational functions in national and international homeopathic professional and educational organisations, and has been a teacher of homeopathy in postgraduate training for doctors.
Since 1998, he has engaged in prognostic factor research (PFR) as an independent researcher. Among other activities, he has performed a prospective PFR study on more than 4,000 patients in 10 practices in the Netherlands. Since 2014, he has been an advisor to the CCRH of the Ministry of AYUSH on PFR.
References
